









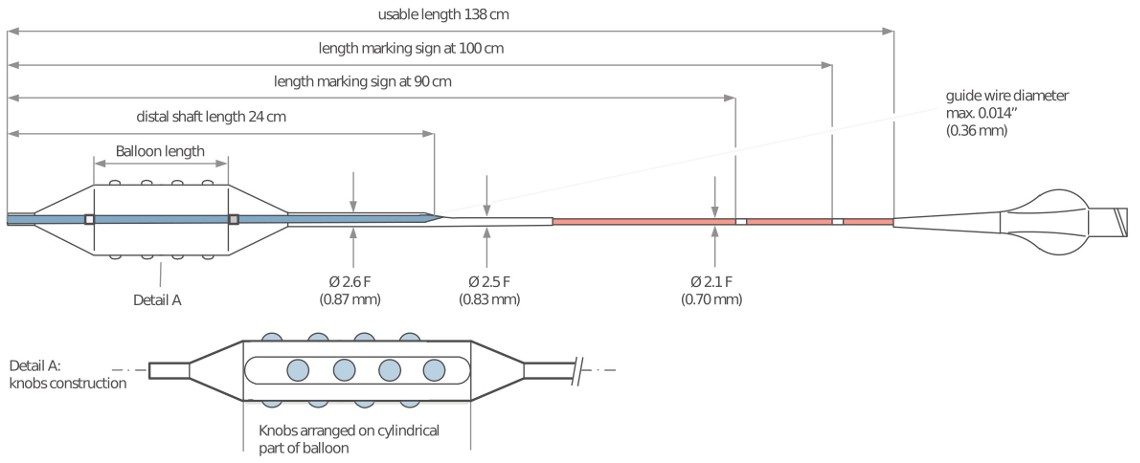
Punta fuerte de 2 mm
Beneficios
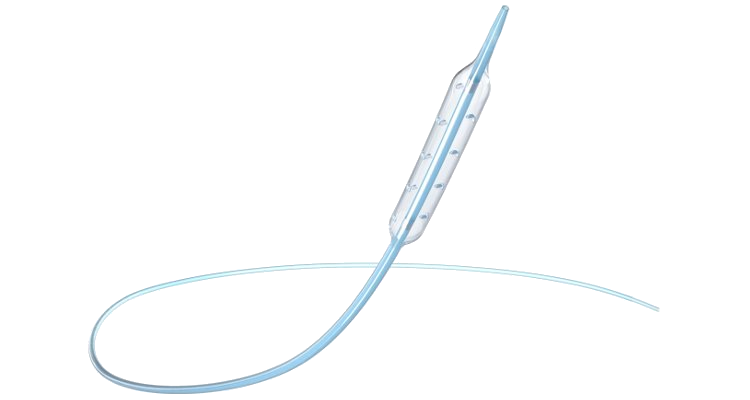
Cuando la reestenosis y la calcificación extrema son una preocupación, GRIP es la solución. With four lines of knobs to crush hard plaque and ensure that the balloon stays where it is placed (minimizing the frustration caused by the watermelon effect), GRIP ofrece estabilidad y resistencia cuando más importa.
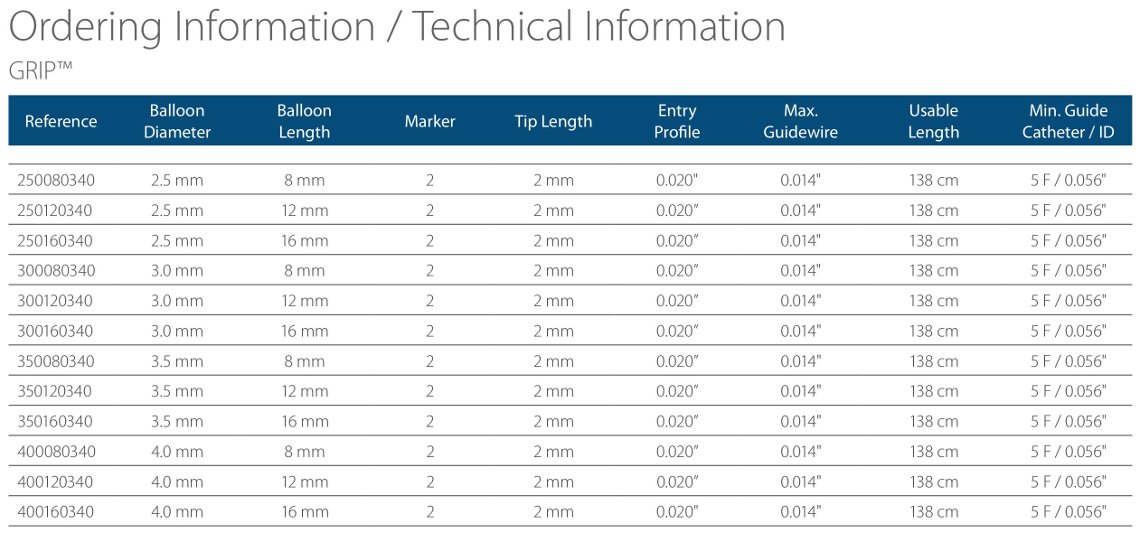
Especificaciones
- Perillas diseñadas para agrietar lesiones muy calcificadas y evitar el deslizamiento.
- Cuatro líneas de perillas fijadas en la superficie resistente del balón.
- Ultra resistente a la perforación.
- Excelente resistencia del material.
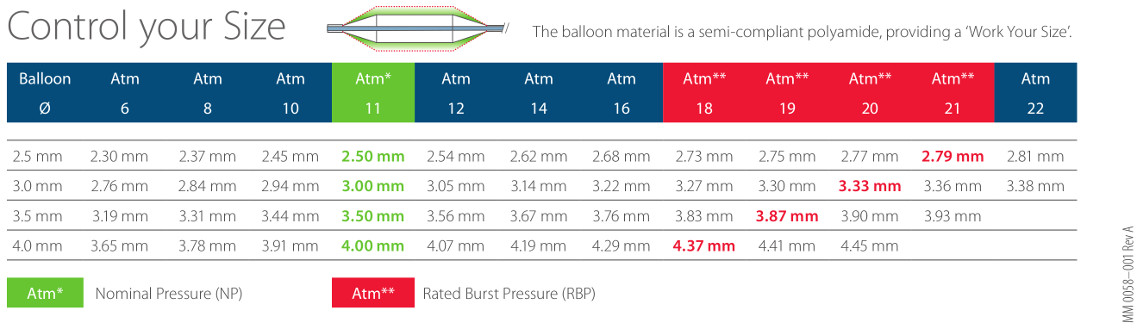
- Alto RBP (hasta 21 atm)
- Punta corta y fuerte (2 mm).
- Estabilidad sin igual con menor riesgo de disección.
Opiniones
About 80% of all restenotic lesions are focal…they are very slippery lesions, very hard.
Almost 100% of all restenotic lesions are treated here with the GRIP balloon.
The use of GRIP balloon with its special knobs gives the opportunity to stabilize the balloon very nicely within the restenotic lesion and to provide enough pressure in the correct place.
The GRIP balloon has a very nice crossing profile, which is very important in treating restenotic lesions.
Dr. Stéphane Cook – Specialist in Cardiology, University Hospital Fribourg – Switzerland
The SVG to RCA presented a very difficult and severely calcified lesion. Pre-dilation was started with a standard NC balloon but several attempts at dilation failed, due to the fact that the balloon slipped away each time dilation was performed.
Balloon dilation was then performed with a GRIP 3.5mm balloon (Acrostak) which was successful on the first attempt. Then a GRIP 4.0mm was dilated up to 30 bar. Thanks to its 4 lines of knobs the GRIP did not slip away and stayed in the lesion area.
After proper balloon dilation with the GRIP balloon, control angiography showed an already good result.
Post dilation with a 4.5mm NC balloon was performed but could not improve the outcome. Acceptable results were achieved.
This procedure shows the efficacy of the GRIP balloon in the treatment of slippery and in-stent restenosis.
Dr. Ahmed Elghamaz – Dept. of Cardiology, Northwick Park Hospital – London, UK
Several predilatations were followed with ACROSS HP 3.0×20, GRIP 3.5x16mm and GRIP 4.0x16mm at 20 atm. A DES was positioned at the ostial RCA and a second DES overlapped the first one in the middle RCA. Post dilatation of mid RCA was performed with a GRIP 3.5x16mm at 22 atm, and the proximal-ostial with a GRIP 4.0x8mm at 20 atm. The GRIP showed great stability for kissing techniques, and was equally effective for pre and post dilatation. Optimal angiographic, functional and IVUS result were achieved.
Dr. Farhat Fouladvand & Dr. Camillo Falcone – Holy Family Hospital & Order of St. John of God Hospital – Erba, Italy
After primary stenting of the DeNovo lesion, pre-dilation was started with Quantum Maverick 3.5x20mm on the lesion area. Several attempts with pressure up to 26 bar failed. We could see the balloon slipping away from the lesion each time which made it impossible to properly dilate the lesion.
The first balloon was replaced by a GRIP balloon 3.5x20mm (Acrostak). The GRIP was dilated up to 28 bar. Thanks to its 4 lines of knobs the GRIP did not slip and instead stayed in the desired lesion area.
The lesion was thus properly dilated after intervening with the GRIP, resulting in a good angiographic outcome.
This procedure shows the superiority of the GRIP over standard balloons when treating slippery and focal in-stent restenosis.
Dr. A Moschovitis – Dept. of cardiology, University Hospital – Bern Switzerland
After usual preparation for angioplasty a 3.0x15mm NC balloon was used to dilate the middle part of the stent, located in the RCA. Several attempts failed despite slow controlled balloon inflations, due to the fact that the balloon slipped away each time dilation was performed.
Balloon dilatation with a GRIP 3.5x12mm balloon (Acrostak) was successful on the first attempt. The GRIP was dilated up to 12 bar.
Thanks to its 4 lines of knobs the GRIP did not slip away and stayed in the lesion area. A repeat angiography, post GRIP balloon dilation, showed good preparation of the vessel.
This case demonstrates the efficacy of the GRIP balloon in the treatment of slippery in-stent restenosis.
Dr. Sohail Q. Khan – Dept. of Cardiology, University Hospitals – Birmingham, UK
The PTCA was initially performed with a 4.0x 12mm Quantum balloon placed on the lesion area. Several attempts with high pressure failed. Each time we could see the balloon slipping away from the lesion which prevented proper dilation.
The first balloon was replaced by a GRIP balloon 3.5x12mm (Acrostak) which was dilated up to 18 bar. The knobs ensured that the GRIP did not slip away and instead stayed in the lesion area.
The lesion was properly dilated after the use of the GRIP with good angiographic results.
This procedure shows the superiority of the GRIP over standard balloons when treating slippery and focal in-stent restenosis.
Dr. A Moschovitis – Dept. of cardiology, University Hospital – Bern Switzerland
The GRIP balloon created a good result in predilating an ISR, thus allowing posterior use of a non-compliant balloon without difficulty.
Dr. De la Torre – Chief of the Hemodynamics Cathlab, Air Force Hospital – Santiago, Chile
{kind=link}